Storia e esame genitourinario - maschile
Revisione paritaria di Dr Philippa Vincent, MRCGPUltimo aggiornamento di Dr Hayley Willacy, FRCGP Ultimo aggiornamento 27 gen 2025
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Aggiungi alle fonti preferite su Google
Professionisti Medici
Gli articoli di riferimento professionale sono progettati per essere utilizzati dai professionisti della salute. Sono scritti da medici del Regno Unito e basati su prove di ricerca, linee guida del Regno Unito ed europee. Potresti trovare uno dei nostri articoli sulla salute più utile.
Despite the increasingly widespread use of imaging of the urinary tract, a thorough history and examination are essential in the assessment of all patients presenting with genitourinary symptoms.
The presentation must be assessed in the context of the age, gender and past medical and surgical history of the patient. Urinary symptoms may not be indicative of urological abnormality but may have other causes such as frequency of micturition in anxiety or urinary symptoms caused by neurological disease.
The following account will both list important items as an aide-mémoire and provide diagnostic tips and suggestions for history and examination. Paediatric genitourinary history and examination are referred to and important aspects particular to developing children are outlined. The separate partner article Genitourinary history and examination -female covers detail specific to female patients.
Male genitourinary history
Care should again be taken to ensure privacy and comfort for both history and examination. Establish confidence and rapport. Allow the patient to describe their complaint or problem. It may be appropriate and necessary to ask details about sexual and psychosexual history. Sign-posting these intimate and personal questions and explaining their importance can facilitate better co-operation from the historian. Specific, closed questioning may be appropriate. Significant symptoms and history are described below.
Sintomi urinari
The history of urinary symptoms should cover the following questions:
Is there disuria?
Is there frequency of micturition? Is there any nocturia?
Is there any terminal dribbling of micturition?
Is there hesitancy of micturition?
How full is the urinary stream?
Have symptoms developed gradually or suddenly?
Is there any incontinenza or urgency of micturition? There may be stress incontinence, detrusor instability, detrusor underactivity or urethral obstruction.
Abnormalities of micturition in men are most often caused by prostatism (see also the separate articles Iperplasia prostatica benigna e Cancro alla prostata). This leads to hesitancy, reduced strength of urine flow and terminal dribbling.
Symptoms of prostatism can be assessed by using the International Prostate Symptom Score (I-PSS) but this does not give an indication of the degree of prostate size or nature of underlying pathology. Complete obstruction may lead to complete inability to pass urine, or to overflow incontinence.
Secrezione uretrale
This is a relatively common presenting symptom. Ask about:
Disuria.
Possible exposure to infezioni sessualmente trasmissibili:
When was contact?
Has the partner had symptoms?
Are there any other symptoms? - for example, with artrite reattiva:
Dolori articolari.
Eye inflammation, pain or grittiness.
Sintomi gastrointestinali.
Testicular pain
This can be an intense pain. Enquiry should be made about:
Trauma.
Speed of onset.
Association with other conditions (for example, mumps).
Other urinary symptoms, such as dysuria or urethral discharge.
Possible causes include trauma, infection, torsion and epididymitis.
Genital ulcers
Genital ulcers are likely to be caused by sexually transmitted infection. Enquiry should be made with this in mind.
Impotence
Impotence covers a number of different conditions and causes. Consider:
Emotional and psychological factors.
Drugs and alcohol.
Any association with other relevant diseases (diabete mellito, neurological disease, cardiovascular disease).
Whether there is:
Subfertilità
This may be primary (no conception) or secondary (past conception). Subfertilità history should cover:
Conception history.
Length of subfertility.
Sexual history:
Timing and frequency of intercourse.
Impotence and ejaculation.
Storia farmacologica.
Medical history:
Conditions affecting erectile function.
Any chemotherapy or cancer treatment.
History of sexual development.
Altri sintomi
Important examples include:
Loin pain; urinary calculi can cause ureteric obstruction and lead to severe loin pain which radiates to the symphysis pubis or testis. The sudden onset of pain in renal colic or acute urinary retention contrasts with the gradual build-up of pain from a renal tumour or the slow development of urine symptoms from outflow obstruction. Ask about associated features such as pain, haematuria or incontinence.
Systemic symptoms of lesione renale acuta oppure malattia renale cronica - eg, anorexia, vomiting, fatigue, pruritus and peripheral oedema.
Recent onset of back pain in an elderly patient may be indicative of cancro alla prostata with bone metastases.
Alcuni pazienti non presentano sintomi, ma vengono riscontrate anomalie nella misurazione della pressione sanguigna o anomalie nelle analisi di routine delle urine, funzione renale o biochimica del siero.
Storia lavorativa
Exposure to chemical carcinogens such as 2-naphthylamine or benzidine in the chemical or rubber industries may induce bladder cancer many years later.
Viaggi all'estero
Travel to Egypt or Africa may result in exposure to schistosomiasi.
Dehydration during a holiday in a hot climate may lead to the development of kidney stones.
Storia familiare
A family history of kidney failure or malattia policistica renale may be relevant to the underlying problem.
Anamnesi patologica remota
Neurological diseases may cause abnormal bladder function - eg, Malattia di Parkinson, sclerosi multipla or cerebrovascular disease.
Any history of kidney disease, ipertensione, diabetes, gotta or past back injury may also be relevant. Abdominal or pelvic surgery can cause denervation injury to the bladder.
Previous surgery - eg, for prostatic hypertrophy.
Ureteric injury may occur in abdominal operations.
Anamnesi farmacologica
Una storia completa dei farmaci attuali e passati è importante.
Past history of analgesic abuse may be a cause of kidney failure.
Dosages of some drugs may need to be adjusted or stopped in kidney failure.
Male genitourinary examination
The genitourinary examination should incorporate a general examination and an abdominal examination.
Esame generale
General sexual development and secondary sexual characteristics.
Note whether there is evidence of gynaecomastia.
Establish whether the patient is distressed due to pain or appearing unwell, suggesting systemic illness and possibly kidney failure.
Note whether there is evidence of liver disease or thyroid disease.
Note whether there is evidence of anaemia.
All patients with urological symptoms should have their blood pressure measured.
Signs of dehydration such as a dry mouth and tongue may indicate kidney failure or polyuria associated with diabetes.
Lymphadenopathy; lymph nodes may be enlarged due to metastatic spread from any urological cancer.
Esame addominale
Abdomen may be distended due to large polycystic kidneys or ascites due to nephritic syndrome oppure sindrome nefrotica. Palpate for an enlarged bladder or an abdominal aortic aneurysm.
The kidneys are examined by bimanual examination with a hand posteriorly lifting up the kidney towards the examining abdominally placed hand.
Tenderness over the kidney should be tested by gentle pressure over the renal angle.
Palpation for renal enlargement or masses. An enlarged kidney usually bulges forwards. In polycystic kidney disease, there may also be hepatomegaly from hepatic cysts.
Percussion for the presence of ascites (shifting dullness) and for an enlarged bladder.
Hernias and hernial orifices.
Auscultation for a renal bruit in renal artery stenosis (heard above the umbilicus, 2 cm to the left or right of the midline and also in both flanks with the patient sitting up).
Penis
The size and shape variation of the normal penis is quite wide. Examination should involve inspection and palpation of:
Prepuce, glans and foreskin - for example, to exclude a fimosi and signs of ipospadia.
The skin should be examined for ulcers and rashes.
The shaft of the penis is examined for plaques of Peyronie's disease.
Secrezione uretrale.
Scrotum
Inspect scrotal skin.
Palpate testes:
The testes should be equal in size, smooth and relatively firm.
Size/volume can be estimated using an orchidometer (see image).
Orchidometer
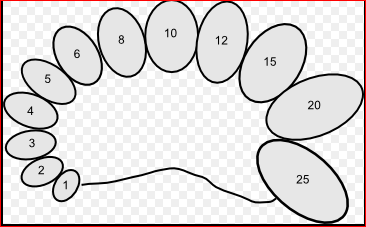
© Filip em (Lavoro proprio) CC BY-SA 3.0, tramite Wikimedia Commons
Small firm testes suggest hypogonadism or testicular atrophy.
Absence of a testis may indicate previous excision, undescended or retractile.
Identify scrotal swellings:
Determine whether it is possible to get above the swelling. With the patient standing, if it is not possible to define the upper border of a mass in the scrotum then it is likely to be an inguinal hernia.
Note whether the swelling is solid or cystic. Note whether there is a hydrocele, varicocele or epididymal cyst. Testing for translucency with a torch will determine whether the mass is cystic or a solid mass. Likely diagnoses are:
Attached to the testis:
Solid (non-translucent): testicular tumour.
Cystic (translucent): hydrocele.
Separate from the testis:
Solid (non-translucent): chronic epididymitis.
Cystic (translucent): epididymal cyst.
Examine the groin and lymphatics.
Prostate
This is examined by rectal examination to assess:
Size.
Consistency.
Any swelling. A hard lump in either or both lobes suggests a cancer and a biopsy is needed to obtain histological proof.
Presence of the medial sulcus.
Any tenderness.
Neurological examination
Dermatome sensory loss of the perineum or lower limbs and lower limb motor dysfunction suggest possible spinal cord or root pathology.
Trauma or compression of the spinal cord may cause urinary retention if acute, or urgency of micturition if a more chronic process.
Acute compression of either the spinal cord or cauda equina may cause bladder and bowel dysfunction and are both neurosurgical emergencies, requiring urgent treatment to prevent irreversible neurological damage.
Storia e esame genitourinario nei bambini
This should involve parents and be done sensitively and carefully. Genitourinary disease in children is more varied and complex (for example, ambiguous genitalia) than in adults. Developmental aspects may be important in both the history and examination. Aspects of this are covered in other separate articles - for example, Pubertà normale e anormale, Storia pediatrica e Esame pediatrico.
Urinary tract infection in children is an important condition which should be diagnosed early and treated adequately if renal scarring is to be avoided in later life.
See the separate article Infezione del tratto urinario nei bambini per maggiori dettagli.
Storia
In general medical practice the history will usually focus on presenting complaints but, in babies particularly, will involve screening for disease as well. Some of the history overlaps with that for adults but an understanding of normal growth and development, particularly of normal pubertal development, is essential in paediatric practice. Child abuse may present with genitourinary symptoms. When child abuse is suspected the correct procedures should be followed with referral for further assessment and examination.
Esame
Again this will be conducted with a good understanding of normal growth and pubertal development. Sensitive handling is essential and, broadly speaking, intrusive and intimate examinations are rarely appropriate. Ultrasound and other investigative techniques can now be used to assess internal organs. Inspection is often all that is required.
Aggiornamenti esclusivi per i professionisti sanitari
Rimani informato con gli ultimi aggiornamenti clinici, approfondimenti professionali e linee guida basate su evidenze. La newsletter Patient Pro seleziona contenuti essenziali per i professionisti sanitari—consegnati direttamente nella tua casella di posta.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.
Ulteriori letture e riferimenti
- Whitfield HN; ABC of urology: Urological evaluation. BMJ. 2006 Aug 26;333(7565):432-5.
- Urological cancers - recognition and referral; NICE CKS, febbraio 2021 (accesso solo Regno Unito)
- Infezione del tratto urinario nei minori di 16 anni: diagnosi e gestione; Linee guida NICE (luglio 2022)
- Infezioni Sessualmente Trasmissibili in Cure Primarie; Royal College of General Practitioners and British Association for Sexual Health and HIV (2013)
Informazioni sull'autoreVisualizza il profilo completo

Dr Hayley Willacy, FRCGP
Medico di base, Autore medico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dott.ssa Hayley Willacy era un medico di base del NHS che lavorava nel nord-ovest dell'Inghilterra, e si è ritirata dalla pratica clinica nel 2022 dopo 30 anni.
Informazioni sul recensoreVisualizza il profilo completo

Dr Philippa Vincent, MRCGP
Medico di base, Autore medico
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent è un medico di base del NHS che lavora nel nord di Londra.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Articolo disponibile anche in Inglese, Tedesco, Spagnolo, Francese, Italiano, Portoghese, Hindi, Ebraico, Arabo, and Svedese.
Prossima revisione prevista: 26 Gen 2028
27 gen 2025 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Più in storia ed esame
- Genitali ambigui
- Monitoraggio ambulatoriale della pressione sanguigna
- Esami prenatali e diagnosi di gravidanza
- AggiornatoAscite
- Dolore toracico
- Dispareunia
- Infezioni fungine delle unghie
- Anamnesi e esame genitourinario - donna
- Esame ginecologico e anamnesi
- Auscultazione cardiaca
- Idrocele
- Allucinazioni ipnagogiche
- Perdita di libido
- Tachicardie a complesso stretto
- Esame pediatrico
- Storia ed esame del sistema respiratorio
- Disturbo da sintomi somatici
- Angioma a fragola
- Svenimento
- Incontinenza urinaria