Retinopatia diabetica
Revisione paritaria di Dr Krishna Vakharia, MRCGPUltimo aggiornamento di Dr Hayley Willacy, FRCGP Ultimo aggiornamento 16 Gen 2024
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Aggiungi alle fonti preferite su Google
If you have diabetes, it is vital that you have your eyes checked regularly. The retina is at the back of the eye and damage to the retina (the light sensitive layer of cells) is called a retinopathy. Retinopathy is a common complication of diabetes.
If left untreated, it can become worse and cause some loss of vision, or total loss of vision (severe sight impairment) in severe cases. Good control of blood sugar (glucose) and blood pressure slows down the progression of retinopathy. Treatment with a laser, before the retinopathy becomes severe, can often prevent loss of vision.
A colpo d'occhio
Diabetic retinopathy is an eye condition affecting blood vessels in the retina, caused by diabetes.
High blood sugar can weaken and damage the tiny blood vessels in the retina over time.
Many people have no symptoms initially, but it can lead to vision loss if untreated.
Regular eye checks, at least once a year, are vital for early detection and treatment.
Treatment like laser therapy can prevent worsening vision but cannot restore lost vision.
Controlling blood sugar, blood pressure, and cholesterol can help prevent retinopathy.
Iscriviti al nostro corso gratuito di 10 settimane sul diabete!
Ogni settimana esploreremo un argomento diverso per aiutarti a comprendere e gestire meglio il tuo diabete, inclusi la vita quotidiana e i farmaci, il benessere mentale, le ultime novità nella tecnologia per il diabete e la nutrizione.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.
What is diabetic retinopathy?
Diabetic retinopathy is a diabetes-related eye condition that affects the blood vessels in the retina.
The term retinopathy covers various disorders of the retina, which can affect vision. Retinopathy is usually due to damage to the tiny blood vessels in the retina.
Retinopathy is commonly caused by diabetes but is sometimes caused by other diseases such as very pressione alta (ipertensione).
Nota: people with diabetes also have a higher risk of developing other eye problems, including cataratta e glaucoma.
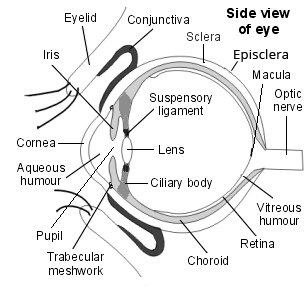
Vista laterale della struttura dell'occhio
How does diabetic retinopathy occur?
Over several years, a high blood sugar (glucose) level can weaken and damage the tiny blood vessels in the retina. This can result in various problems which include:
Small blow-out swellings of blood vessels (microaneurysms).
Small leaks of fluid from damaged blood vessels (exudates).
Small bleeds from damaged blood vessels (haemorrhages).
Blood vessels may just become blocked. This can cut off the blood and oxygen supply to small sections of the retina.
New abnormal blood vessels may grow from damaged blood vessels. This is called proliferative retinopathy. These new vessels are delicate and can bleed easily.
The leaks of fluid, bleeds and blocked blood vessels may damage the cells of the retina. In some severe cases, damaged blood vessels bleed into the jelly-like centre of the eye (the vitreous humour). This can also affect vision by blocking light rays going to the retina.
Diabetic retinopathy symptoms
Initial symptoms that may occur include:
Visione offuscata.
Seeing floaters and flashes.
Having a sudden loss of vision.
Most people with diabetic retinopathy do not have any symptoms or visual loss due to their retinopathy. However, without treatment, diabetic retinopathy can gradually become worse and lead to visual loss or even total loss of vision (severe sight impairment).
Different parts of the retina can be affected.
The macula is a small part of the retina which is roughly in the centre at the back of the eye. The macula is where you focus your vision. So, when you read or look at an object, the light focuses on the macula. The central and most important part of the macula is called the fovea.
The outer part of the retina is used for peripheral vision.
Retinopathy can affect the macula, the outer part (peripheral) of the retina, or both. It is much more serious if the macula is affected.
Diabetic retinopathy stages
Retinopathy usually develops gradually and tends to become worse over a number of years:
Stage 1: background retinopathy
Background retinopathy does not change your sight. With this you have some tiny leaks of fluid and tiny bleeds (microaneurysms) in various parts of the retina. A doctor or optometrist can see these as tiny dots and blots on the retina when they examine the back of the eye.
Stage 2: pre-proliferative retinopathy
Pre-proliferative retinopathy is more extensive than background retinopathy. There are signs of blood flow becoming restricted but not yet showing new blood vessels growing (see below).
Stage 3: proliferative retinopathy
Proliferative retinopathy is the advanced diabetic retinopathy that occurs when damaged blood vessels in the retina make chemicals called growth factors. These can cause new tiny blood vessels to grow (proliferate) from the damaged blood vessels. This is an attempt to repair the damage.
However, these new blood vessels are not normal. They are delicate and can easily bleed, obscuring your vision. In this type of retinopathy, without laser treatment, vision is likely to become badly affected.
If the proliferative retinopathy becomes severe then many abnormal new blood vessels grow. They may block the drainage channels in your eye, causing increased pressure in the eye (glaucoma), or accompanying fibre growth may cause the retina to detach from the back of the eye.
The effects of retinopathy may be different in each eye. Also, if you have high blood pressure (hypertension) in addition to diabetes, it can make retinopathy worse or progress more quickly.
Who develops diabetic retinopathy?
Retinopathy is a common complication of diabetes. It is more common in people with diabete di tipo 1. Diabetic retinopathy is the most common cause of severe sight impairment in people of working age in the UK.
Fattori di rischio
Risk factors for diabetic retinopathy include:
Duration of diabetes. The longer you have had diabetes, the higher your risk of developing retinopathy. It is uncommon if you have had diabetes for less than five years. However, around 9 in 10 people who have had diabetes for longer than 30 years can be affected.
Poor blood sugar (glucose) control. Studies have shown that those people with poor control of their diabetes are more likely to develop all complications, including retinopathy. However, one large study has shown that even a proportion of people who have very well controlled glucose levels still develop diabetic retinopathy in the future.
Alta pressione sanguigna (ipertensione). If your blood pressure is not well controlled then this will increase your risk of developing retinopathy.
Kidney disease (nephropathy). Having kidney disease as a result of your diabetes is associated with worsening retinopathy.
Gravidanza. Being pregnant may make retinopathy worsen, especially if your blood glucose is poorly controlled.
Other risk factors include smoking, obesity and having a high cholesterol level.
Eye checks for diabetic retinopathy
NICE guidance on screening and referral for diabetic eye problems
The National Institute for Health and Care Excellence (NICE) has updated two of its recommendations about eyes for people with diabete di tipo 2. It recommends that:
As soon as you are diagnosed with type 2 diabetes, you should be referred to the local eye screening service for the checks below.
If your vision suddenly becomes significantly worse, you should be referred to a specialist eye doctor (an ophthalmologist). How urgently you are referred depends on your personal circumstances, but it is important to contact your GP promptly if this happens.
Treatment can prevent loss of vision in most cases. Therefore, if you have diabetes, it is vital that you have regular eye checks to detect retinopathy before your vision becomes badly affected. You should have an eye check at least once a year.
The annual screening test should include:
Testing your vision.
Taking digital photographs of your retina (to compare with previous examinations).
To examine your eyes properly you will have drops put into your eyes to make the pupil as wide as possible. The drops can make your vision blurry for up to six hours. This can affect your ability to drive so you should not drive to or from the place where the test is carried out.
Another test which is sometimes done at the eye hospital, when retinopathy is suspected, is a fluorescein angiogram. This involves having a special dye injected into one of the veins in your arm. This dye then travels to the blood vessels in your eye. A camera with a special filter is used to show up any swollen, leaking or abnormal blood vessels.
If you are found to have no retinopathy or mild (background) retinopathy, and your vision is not affected, you are likely just to be invited back for screening in 12 months' time. The retinopathy may not progress to more serious forms, particularly if your diabetes and blood pressure are well controlled. If more severe changes are detected, you may be referred to an eye specialist for a detailed eye examination, and treatment if necessary.
Even if your check shows you do not have any retinopathy then you should still look after your diabetes and have a healthy lifestyle to reduce the risk of a retinopathy developing in the future.
Nota: if you notice any change in your vision before you are due a routine check, arrange to have an eye check earlier.
What is the treatment for diabetic retinopathy?
If you have mild diabetic retinopathy then you will not usually require any treatment other than controlling any other risk factors (for example, blood pressure, blood sugar (glucose) and cholesterol levels).
The main treatment options for diabetic retinopathy are:
Trattamento laser
Laser treatment is used mainly if you have new vessels growing (proliferative retinopathy), or if any type of retinopathy is affecting the macula. A laser is a very bright light that is very focused so it makes tiny burns on whatever it is focused on.
A burn can seal leaks from blood vessels, and stop new vessels from growing further. The burns are so tiny and accurate that they can treat a tiny abnormal blood vessel. Several hundred burns may be needed to treat retinopathy.
There are different types of lasers. The type chosen may depend upon your actual eye condition. It is common to need several treatment sessions.
Treatment usually works well to prevent retinopathy from getting worse, and so often prevents loss of vision. However, laser treatment cannot restore vision that is already lost.
You may find after your laser treatment that your sight may become dim or blurred. This normally improves over the following few days.
Altri trattamenti
Various eye operations may be needed if you have a bleed into the jelly-like centre of the eye (the vitreous humour) or develop a detached retina.
These are possible consequences of severe retinopathy. An operation may also occasionally be needed if your laser treatment has not been successful.
Diabetic macular oedema
A complication of diabetic retinopathy is diabetic macular oedema. The macula is on the retina so this is also a type of retinopathy and is similar to wet age-related macular degeneration.
In diabetic macular oedema, the leaky vessels in the macula can cause fluid build-up (oedema). Initially, there may not be a change in vision but over time your central vision can become blurred. Diabetic macular oedema is the leading cause of registered blindness in the UK.
The treatment for this includes laser therapy and surgery. However, there are also injections containing anti-vascular growth factors (anti-VEGF) that can be given to improve vision.
VEGF is a chemical that is involved in the formation of new blood vessels in the macula. By blocking the action of this chemical, it helps prevent the condition from progressing and may partially reverse it.
Anti-VEGF medicines include ranibizumab and aflibercept. These are usually the first-line treatments. NICE has just advised of another that works just as well called faricimab - see Further Reading and References below.
There are specific criteria for these medications and if you are eligible, your doctor will discuss them with you.
Can diabetic retinopathy be prevented?
You are less likely to develop retinopathy or, if you have mild (background) retinopathy it is less likely to progress to more serious retinopathy, if:
You control your blood sugar (glucose) levels. Treatment to control blood glucose is discussed in other leaflets on diabetes. Briefly, it involves a dieta sana, losing weight if you are overweight, regular exercise and medication if required.
Your blood pressure and cholesterol levels are well controlled.
Some studies also suggest that smoking may make retinopathy worse. Therefore, you are also advised to smettere di fumare if you smoke.
Scelte del paziente per Vivere con il diabete

Diabete
Gestire l'iperglicemia
Questo opuscolo è stato creato sulla base dei consigli di primo soccorso forniti da St John Ambulance, la principale organizzazione di primo soccorso del paese. Questi consigli non sostituiscono la formazione di primo soccorso - cerca un corso di formazione vicino a te.
da St John Ambulance

Diabete
Diabete e malattia
Se hai il diabete - o devi prenderti cura di qualcuno che ce l'ha - è importante essere preparati a gestire la malattia. Non esitare a contattare il tuo medico o infermiere se hai bisogno di consigli o supporto.
di Dr Colin Tidy, MRCGP
Domande frequenti
What is the fovea, and why is it important for my vision?
The fovea is the central and most crucial part of the macula, which is a small area in the middle of your retina. The macula is responsible for your central vision, meaning it's where light focuses when you're reading or looking directly at an object. If the fovea is affected by retinopathy, it can significantly impact your ability to see clearly and focus.
How urgently should I seek medical attention if my vision suddenly worsens?
If you experience a sudden and significant worsening of your vision, you should contact your GP promptly. Depending on your personal circumstances, you should be referred to a specialist eye doctor (an ophthalmologist) urgently. It's also important to arrange an eye check earlier if you notice any changes in your vision before your next routine appointment.
Will laser treatment restore lost vision?
Laser treatment is generally very effective at preventing diabetic retinopathy from getting worse and can prevent further loss of vision. However, it cannot restore vision that has already been lost due to the condition. Its primary purpose is to seal leaks and stop the growth of new, abnormal blood vessels.
What is a fluorescein angiogram, and when might I need one?
A fluorescein angiogram is a specialized test sometimes performed at an eye hospital when retinopathy is suspected. It involves injecting a special dye into a vein in your arm, which then travels to the blood vessels in your eye. A camera with a special filter is used to highlight any swollen, leaking, or abnormal blood vessels, helping eye specialists assess the extent of the damage.
How long will my vision be blurry after having eye drops for a diabetic eye check?
When you have eye drops administered to widen your pupils for a proper eye examination, your vision can be blurry for up to six hours afterwards. Because of this, it's advised not to drive yourself to or from the appointment.
Ulteriori letture e riferimenti
- Diabete di tipo 1 negli adulti: diagnosi e gestione; Linee guida NICE (agosto 2015 - ultimo aggiornamento agosto 2022)
- Diabete (tipo 1 e tipo 2) nei bambini e nei giovani: diagnosi e gestione; Linee guida NICE (Ago 2015 - aggiornato Mag 2023)
- Diabete di tipo 2 negli adulti: gestione; Linee guida NICE (dicembre 2015 - ultimo aggiornamento giugno 2022)
- Faricimab per il trattamento dell'edema maculare diabetico; Linee guida di valutazione tecnologica NICE, giugno 2022
- Brolucizumab per il trattamento dell'edema maculare diabetico; Linee guida di valutazione tecnologica NICE, agosto 2022
- Tan TE, Wong TY; Diabetic retinopathy: Looking forward to 2030. Front Endocrinol (Lausanne). 2023 Jan 9;13:1077669. doi: 10.3389/fendo.2022.1077669. eCollection 2022.
- Tan CH, Kyaw BM, Smith H, et al; Use of Smartphones to Detect Diabetic Retinopathy: Scoping Review and Meta-Analysis of Diagnostic Test Accuracy Studies. J Med Internet Res. 2020 May 15;22(5):e16658. doi: 10.2196/16658.
Informazioni sull'autoreVisualizza il profilo completo

Dr Hayley Willacy, FRCGP
Medico di base, Autore medico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dott.ssa Hayley Willacy era un medico di base del NHS che lavorava nel nord-ovest dell'Inghilterra, e si è ritirata dalla pratica clinica nel 2022 dopo 30 anni.
Informazioni sul recensoreVisualizza il profilo completo

Dr Krishna Vakharia, MRCGP
Direttore Sanitario per la Salute, Optum UK
MBChB, MRCGP(2013), BMedSci (hons), DFSRH, DRCOG, PGDipDerm (Distn)
La Dott.ssa Krishna Vakharia è un medico di base del NHS. È anche un'esaminatrice regolare per il Diploma post-laurea in Dermatologia Pratica presso l'Università di Cardiff, oltre ad essere il Direttore Medico per la salute presso Optum UK.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Articolo disponibile anche in Inglese, Tedesco, Spagnolo, Francese, Italiano, Portoghese, Hindi, Ebraico, Arabo, and Svedese.
Prossima revisione prevista: 14 Gen 2029
16 Gen 2024 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Iscriviti alla newsletter di Patient
La tua dose settimanale di consigli sulla salute chiari e affidabili - scritti per aiutarti a sentirti informato, sicuro e in controllo.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.
Di più sul diabete
- Gestire l'iperglicemia
- Diabete
- Diabete e ipertensione
- Diabete e malattia
- Diabete e gravidanza
- Diabete nei bambini
- Amiotrofia diabetica
- Ulcere del piede diabetico
- Malattia renale diabetica
- Neuropatia diabetica
- Guida e diabete
- Test di tolleranza al glucosio
- Convertitore HbA1c
- Ipoglicemia
- Insulina
- Diabete di tipo 1
- Diabete di tipo 2
- Dieta per il diabete di tipo 2
- Trattamento del diabete di tipo 2