Sterilizzazione femminile
Revisione paritaria di Dr Hayley Willacy, FRCGP Ultimo aggiornamento di Dr Toni Hazell, MRCGPUltimo aggiornamento 19 maggio 2023
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Aggiungi alle fonti preferite su Google
In questa serie:SterilizzazioneVasectomia
La sterilizzazione femminile è un metodo contraccettivo. È una procedura eseguita per impedire agli ovuli di raggiungere gli spermatozoi.
A colpo d'occhio
Female sterilisation is a permanent contraceptive method.
It involves cutting or blocking the Fallopian tubes to prevent eggs from reaching sperm.
The procedure usually takes about 20 minutes and is often done as a day-case.
It is 99.5% effective, meaning 1 in 200 women may become pregnant within a year.
Recovery from a keyhole procedure typically takes a few days.
Sterilisation does not protect against sexually transmitted infections.
If you have pain or unexplained bleeding after sterilisation, see a doctor quickly.
How is female sterilisation done?
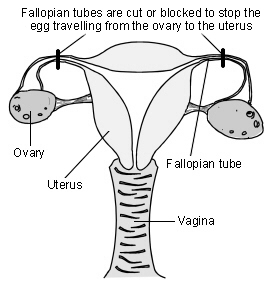
The tubes between the ovary and the womb (the Fallopian tubes) are cut or blocked with rings or clips. This stops the eggs which are released by the ovary from reaching the sperm.
Female reproductive organs
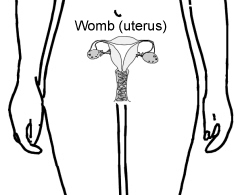
Diagram showing how female sterilisation is performed
The operation is usually done under general anaesthetic but can be done with a local or regional anaesthetic while you are awake. For most women the operation is done with the help of a special telescope called a laparoscope.
The laparoscope is inserted through a very small cut in your tummy (abdomen). It allows the surgeon to see what they are doing. Another small cut is then made to insert an instrument to block the tubes. A number of ways are used to do this. Most often clips or rings are applied to your tubes. The clips or rings provide a block in the tubes and prevent the egg from meeting sperm.
A larger cut may have to be made, and a more traditional operation done, in some women. This is more likely if laparoscopia is too risky, such as if you have had multiple previous operations, or if you are overweight. This is called a mini-laparotomy.
If blocking the Fallopian tubes doesn't work then either part or all of the tubes can be removed. This is called a salpingectomy.
Sterilisation can be performed at the same time as a taglio cesareo, when a segment of the tube is removed. This is done after the delivery of the baby. It has a higher failure rate than a sterilisation which is not done at the time of caesarean delivery.
How long does the procedure take?
The procedure itself usually takes about 20 minutes, and should be done as a day-case, so you arrive at hospital early in the morning and go home the same day (unless there are unexpected complications).
How reliable is female sterilisation?
The failure rate of female sterilisation is 0.5%, so 1 in 200 women will get pregnant within one year As a comparison, when no contraception is used, more than 800 out of 1,000 sexually active women will become pregnant within one year. This failure rate is much higher than for some long-acting reversible contraceptive (LARC) methods (for example only 1 woman in 2000 will get pregnant per year on the implant) and so a LARC should always be offered to a woman who is considering sterilisation.
After sterilisation, women can become pregnant if the tubes come back together again after being cut. If clips were used to block the tubes, the clips can occasionally work their way off - even when they have been put on correctly.
Advantages of female sterilisation
Do you still have periods after being sterilised?
It is permanent and you (and your partner) don't have to think about contraception again. There are no hormones involved, so you do not have the side-effects of many other types of contraception.
Disadvantages of female sterilisation
Sterilisation is permanent and very difficult to reverse. Some women may regret having the operation in future years, particularly if their circumstances change. Periods may become heavier after sterilisation - sometimes this is because you have stopped using another method, such as the pill, which lightens your periods, but it can also happen if you have not moved from another method.
In the rare event that the procedure fails and you become pregnant, you are more likely to have an gravidanza ectopica. This occurs when the pregnancy develops outside of the womb, usually in the Fallopian tube. You would need emergency treatment if this were to happen. If you think you are pregnant after a sterilisation, or have unexplained bleeding or pain in your tummy (abdomen), then see a doctor quickly.
Laparoscopic sterilisation is also not as easy to do or as effective as male sterilisation (vasectomy). There is a small risk from the insertion of the laparoscope which has to be done 'blind' (ie without any image guidance). This means the surgeon cannot see exactly where they are putting the instrument in the tummy to gain access to the tubes.
It may at times damage organs like bowel or a blood vessel inside the abdomen. This sounds worrying. However, the surgeon takes many precautions to make the procedure safe and to avoid causing damage to any other organ and, in most cases, this does not happen.
Sterilisation doesn't protect against sexually transmitted infection (STIs) so you may need to use condoms if you think you may be at risk of STI.
As with any operation there is a risk of a wound infection and the slight risk from a general anaesthetic. There may be some tummy discomfort or bloating, or mild discomfort or pain at the site of the cut.
How soon is female sterilisation effective?
For laparoscopic sterilisation it depends on when you have it done in your menstrual cycle. If it is done whilst you have your period, you will not have produced an egg yet. In this case the procedure is effective immediately.
At any other time in your cycle, you will usually be advised to continue your previous method of contraception until your next period.
(The procedure is only done after checking you are not pregnant. That is, a pregnancy test would be done. If you have had sex without using contraception in the previous three weeks it is not possible to be sure you will not be pregnant. In this case, the operation would be delayed.)
Does female sterilisation affect sex drive?
No. Sex may seem more enjoyable, as the worry of pregnancy and contraception is removed.
How long does it take to recover from female sterilisation?
It usually takes a few days to recover from a laparoscopic sterilisation and most people can return to work within five days, but should avoid heavy lifting for a week. If a mini-laparotomy (open surgery rather than keyhole) was needed then recovery will be longer, and you may need to be off work for 3-4 weeks and avoid heavy lifting for 6 weeks. It is always important to care for yourself after surgery.
Points to consider
Don't consider having the operation unless you and your partner are sure you do not want children, or further children. It is wise not to make the decision at times of crisis or change - for example, after a new baby or termination of pregnancy. Don't make the decision if there are any major problems in your relationship with your partner. It will not solve any sexual problems.
Doctors normally like to be sure that both partners are happy with the decision before doing this permanent procedure. However, it is not a legal requirement to get your partner's permission. If you have any doubts and questions, make sure you discuss these with your doctor or practice nurse.
Have you considered the alternatives? Female sterilisation is not 100% effective. Other reversible methods of contraception are often more effective, such as the intrauterine system (IUS), contraceptive implants e contraceptive injections. Also, male sterilisation is easier and safer to do and is more effective.
Scelte del paziente per Altri interventi chirurgici e procedure

Chirurgia e procedure
Artroscopia e chirurgia artroscopica
L'artroscopia è una procedura chirurgica che utilizza un sottile telescopio con una fonte di luce (artroscopio) per osservare l'interno delle articolazioni. Oltre a poter guardare all'interno, il chirurgo può usare un artroscopio per eseguire interventi minimali. L'artroscopia viene più spesso utilizzata per indagare o trattare problemi al ginocchio. Può essere utilizzata anche per altre articolazioni, tra cui spalla, anca, gomito, polso e caviglia, e persino per problemi alla mano o al piede. Nota: le informazioni di seguito sono solo una guida generale. Le modalità e il modo in cui vengono eseguiti i test possono variare tra diversi ospedali. Seguire sempre le istruzioni fornite dal proprio medico o dall'ospedale locale.
di Dr Rachel Hudson, MRCGP
Chirurgia e procedure
Chirurgia per menorragia
I cicli mestruali abbondanti sono comuni. Nella maggior parte dei casi non si trova una causa. In alcuni casi si trova una causa come l'endometriosi o i fibromi. Nella maggior parte dei casi il trattamento è efficace utilizzando farmaci o un sistema intrauterino (IUS) per ridurre il sanguinamento. Tuttavia, alcune donne avranno bisogno di un intervento chirurgico. Qui verranno discussi i diversi tipi di interventi chirurgici disponibili.
di Dr Colin Tidy, MRCGP
Domande frequenti
What is the advantage of sterilisation compared to other methods of contraception?
The main advantage of female sterilisation is that it is permanent, meaning you and your partner do not have to think about contraception again. Additionally, it involves no hormones, so you avoid the side-effects associated with many other types of hormonal contraception.
Is female sterilisation a completely safe procedure?
While surgeons take many precautions to ensure safety, there are some risks associated with female sterilisation. These include a small risk of damage to organs like the bowel or blood vessels during the insertion of the laparoscope. As with any operation, there's also a risk of wound infection and a slight risk from general anaesthesia. There might be some temporary tummy discomfort, bloating, or pain at the incision site.
Does female sterilisation offer protection against sexually transmitted infections (STIs)?
No, female sterilisation does not protect against sexually transmitted infections. If you believe you may be at risk of STIs, you will still need to use condoms.
Are there any specific situations where the decision to have a sterilisation should be delayed?
It is advised not to make the decision to have a sterilisation during times of crisis or significant life changes, such as after a new baby or a termination of pregnancy. Also, if there are major problems in your relationship, it is recommended to delay the decision. The procedure should not be undertaken with the expectation that it will resolve sexual problems.
Who typically makes the decision for female sterilisation, and is a partner's consent required?
While doctors usually prefer that both partners are in agreement with the decision due to the permanent nature of the procedure, it is not a legal requirement to obtain your partner's permission for female sterilisation.
Ulteriori letture e riferimenti
- Trussell J; Fallimento contraccettivo negli Stati Uniti, Contraccezione, 2011
- Sterilizzazione maschile e femminile; Facoltà di Salute Sessuale e Riproduttiva (Settembre 2014)
- Contraception - sterilization; NICE CKS, Maggio 2021 (accesso solo UK)
Informazioni sull'autoreVisualizza il profilo completo

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
La Dott.ssa Toni Hazell si è laureata presso la St. Mary’s Hospital Medical School e ha completato il suo VTS al Northwick Park Hospital.
Informazioni sul recensoreVisualizza il profilo completo

Dr Hayley Willacy, FRCGP
Medico di base, Autore medico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dott.ssa Hayley Willacy era un medico di base del NHS che lavorava nel nord-ovest dell'Inghilterra, e si è ritirata dalla pratica clinica nel 2022 dopo 30 anni.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Articolo disponibile anche in Inglese, Tedesco, Spagnolo, Francese, Italiano, Portoghese, Hindi, Ebraico, Arabo, and Svedese.
Prossima revisione prevista: 12 maggio 2028
19 maggio 2023 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Iscriviti alla newsletter di Patient
La tua dose settimanale di consigli sulla salute chiari e affidabili - scritti per aiutarti a sentirti informato, sicuro e in controllo.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.
Di più su chirurgia e procedure
- Riduzione del seno
- Sollevamento del seno
- Broncoscopia
- Aspirazione con ago transbronchiale guidata da ecografia endobronchiale
- Biopsia endometriale
- Sollievo dal dolore epidurale dopo l'intervento chirurgico
- ERCP
- Gastroscopia
- Sostituzione dell'anca
- Isterectomia
- Isteroscopia
- Trapianto di rene
- Sostituzione del ginocchio
- Rimozione dei peli con laser
- Aumento delle labbra
- Nasoendoscopia
- Danno ai nervi dopo iniezione epidurale
- Infezione toracica post-operatoria
- Nausea dopo anestesia
- Addominoplastica