Polipi intestinali
Polipi del colon
Revisione paritaria di Dr Colin Tidy, MRCGPUltimo aggiornamento di Dr Toni Hazell, MRCGPUltimo aggiornamento 15 Set 2023
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Add to preferred sources on Google
In questa serie:Cancro intestinaleScreening del cancro intestinaleTest immunochimico fecaleSigmoidoscopiaColonscopiaColonografia TC
I polipi intestinali (polipi colici) sono piccole escrescenze non cancerose (benigne) sulla mucosa interna dell'intestino (colon e retto).
In questo articolo:
Video picks for Problemi intestinali
Continua a leggere sotto
What are bowel polyps?
A bowel polyp is a small non-cancerous growth. There are many types of polyps, such as those that occur in the nose - this leaflet is about polyps that occur in the bowel.
Types of bowel polyps
Torna ai contenutiLarge bowel - polyp
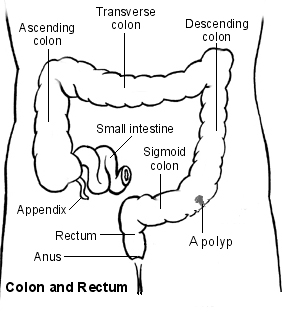
Most bowel polyps develop in the part of the colon called the descending colon, which leads down to the rectum. However, they can occur anywhere in the colon or rectum. Bowel polyps can be divided into three types: hyperplastic polyps, adenomas and polyposis syndromes.
Hyperplastic bowel polyps
These are a common type of bowel polyps. They are small - usually less than half a centimetre in diameter. They are generally regarded as harmless and only very rarely turn into cancer.
Adenomi
These too are a common type of bowel polyp. Most are small (usually less than a centimetre in diameter) but they can be bigger. There is a small risk that an adenoma may, in time, become cancerous. If one does turn cancerous, the change usually takes place after a number of years.
The relationship between polyps and cancer is that most bowel cancers (colorectal cancers) develop from a polyp that has been present for 5-15 years. In other words, although most adenomas do not become cancerous, the vast majority of cancers in the bowel initially develop from an adenoma that has been present for a number of years.
It is difficult to be certain of the exact risk of developing cancer from an adenoma. One study suggested that for a single 1 cm adenoma, the risk of it turning cancerous was about 1 in 12 after 10 years, and about a 1 in 4 after 20 years. However, the risk seems to vary depending on factors such as the size of the adenoma and the exact type of adenoma.
There are different types of adenoma and some types are more likely than others to develop into bowel cancer. See also the separate leaflet on Bowel Cancer Screening.
Polyposis syndromes
Polyposis syndromes are a group of inherited conditions. They include:
Poliposi adenomatosa familiare (FAP).
Hereditary nonpolyposis colorectal cancer (HNPCC)/Lynch's syndrome.
Gardner's syndrome.
Turcot's syndrome.
Sindrome di Peutz-Jeghers.
Cowden's disease.
Familial juvenile polyposis.
Hyperplastic polyposis.
These are rare syndromes. They cause polyps in young people and often cause multiple bowel polyps that have a high chance of developing into bowel cancer.
Continua a leggere sotto
Bowel polyp symptoms
Torna ai contenutiMost people with one or more bowel polyps do not have any symptoms. Most people who have a bowel polyp will never know they have one.
However, some people with bowel polyps will get symptoms. Polyps do not usually cause abdominal pain or a change in bowel habits. Symptoms include:
Blood in the stools (faeces). There may also be mucus in the stools.
Diarrea oppure constipation, but this is much less likely than blood in the stools. Diarrhoea or constipation is much more likely to have a cause other than a bowel polyp.
Causes of bowel polyps
Torna ai contenutiThe lining of the bowel constantly renews itself throughout our lives. New cells are made in the lining of the bowel and these cells eventually die to be replaced by more new cells. Each of these cells contains genes which control how the cell works.
Family history may play a role, because if the gene doesn't work properly then some cells may grow more quickly. This may eventually cause a polyp to develop. Some faulty genes cause a tendency for the lining of the bowel to develop polyps or bowel cancer, which may be inherited from our parents.
Continua a leggere sotto
How common are bowel polyps?
Torna ai contenutiBowel polyps are really common in older people. About 1 in 4 people over the age of 50 years develop at least one colonic polyp. Bowel polyps are much less common in younger people.
Some people develop just one bowel polyp. It is not uncommon to have two or more. However, having more than five polyps is unusual.
Fattori di rischio
Risk factors include increasing age, being overweight and smoking. If you have a family history of a bowel polyp or cancer, or have had either of these yourself in the past, you are also at higher risk. Another risk factor is having inflammatory bowel disease (ulcerative colitis or Crohn's disease).
Diagnosing bowel polyps
Torna ai contenutiMost bowel (colonic) polyps do not cause symptoms. So, most people with bowel polyps will not be diagnosed. Screening tests may be done if you have symptoms that indicate a bowel problem, or for various other reasons. For example, if you have seen blood in your stools (faeces) or if you are found to have blood in your stools following a routine screening test which is now offered to older people.
See the separate leaflet called Faecal Occult Blood Test for more details.
What is a colonoscopy?
Most bowel polyps are diagnosed by this procedure. Colonoscopy is a test where an operator - a doctor or a nurse - looks into your colon. A colonoscope is a thin, flexible telescope. It is about as thick as a little finger. It is passed through the anus and into the colon. It can be pushed all the way around the colon as far as the caecum (where the small and large intestine meet). The colonoscope contains fibre-optic channels which allow light to shine down so the operator can see inside your colon.
Vedi l'opuscolo separato chiamato Colonscopia per maggiori dettagli.
A sample (biopsy) will be taken at the time of the colonoscopy. This is very important so that it can be checked whether the polyp is cancerous (malignant).
What about other tests?
Sometimes a bowel polyp is diagnosed by other tests:
A special X-ray test of the bowel - this procedure is called a barium enema.
A CT colonogram - air and a contrast dye are pumped into the bowel to make the anatomy clearer to see and you are then examined by a CT scanner.
A test procedure called sigmoidoscopia - this enables a doctor or nurse to use an instrument called a sigmoidoscope to look into the rectum and sigmoid colon. The procedure is similar to a colonoscopy but it uses a shorter telescope.
If a bowel polyp is seen on a barium enema or CT colonogram you will still need a colonoscopy to remove the polyp and to take a sample (biopsy) of it for further investigation. The advantage of a colonoscopy as the first test is that the biopsy can be taken and/or the polyp removed all at the same time.
You will also need a colonoscopy if a polyp is found when you have a sigmoidoscopy. This is to make sure there are no more polyps beyond the reach of sigmoidoscopy.
Treatments for bowel polyps
Torna ai contenutiIf you are diagnosed with a bowel polyp, you will usually be advised to have it removed, even if it is not causing any symptoms. This is because there is a small risk of the polyp developing into a cancerous (malignant) growth at some time in the future.
Colonscopia
Most bowel polyps can be removed during a colonoscopy. The colonoscope has a side channel down which a grabbing device can be passed. This device can be manipulated by the operator. The operator can therefore see and also remove a polyp during a colonoscopy. The removal of the polyp is usually painless. Once removed, the bowel/colon polyp is sent to the laboratory to be looked at under a microscope. This is done to check:
That it has been completely removed.
The type of polyp.
Whether it is non-cancerous (benign) or showing signs of cancerous (malignant) change.
Most removed polyps will show full removal and be totally benign.
Your consultant will advise on the need for follow-up. This may depend on factors such as the size of the bowel polyp, the exact type of polyp that has been removed, the laboratory report about the polyp, and your age. Once these factors are considered, some people are advised to have regular colonoscopies in the future to make sure no more bowel polyps develop. As with any test, the results should be given to you by the team who arranged the test. So if you are not sure about how to access the results, phone or email your consultant's secretary, not your GP.
Chirurgia
If you have many bowel polyps (especially if you have a polyposis syndrome) then you may need to have an operation to remove part of your bowel. This is because it isn't possible to completely remove all the bowel polyps by using colonoscopy.
Preventing bowel polyps
Torna ai contenutiPolyps cannot be prevented, but a healthy lifestyle (not smoking and not being overweight) can help to reduce your risk.
Patient picks for Problemi intestinali

Salute digestiva
Sindrome dell'intestino irritabile
IBS sta per sindrome dell'intestino irritabile, ed è una condizione cronica a lungo termine dell'intestino che provoca episodi di crampi addominali, gonfiore e stitichezza o diarrea. L'IBS è un problema legato al funzionamento dell'intestino.
di Dr Rachel Hudson, MRCGP

Salute digestiva
Costipazione
La stitichezza significa che stai evacuando meno del normale, hai difficoltà a defecare o hai evacuazioni dolorose. Di solito è causata da un insufficiente apporto di fibre o da una scarsa assunzione di liquidi.
by Dr Caroline Wiggins, MRCGP
Ulteriori letture e riferimenti
- Combined endoscopic and laparoscopic removal of colonic polyps; NICE Interventional procedures guidance, September 2014
- Cancro colorettale (gestione nelle persone di età pari o superiore a 18 anni); Linee guida NICE (2020, ultimo aggiornamento dicembre 2021)
- Screening intestinale; NICE CKS, maggio 2019 (accesso solo Regno Unito)
- Bonnington SN, Rutter MD; Surveillance of colonic polyps: Are we getting it right? World J Gastroenterol. 2016 Feb 14;22(6):1925-34. doi: 10.3748/wjg.v22.i6.1925.
Continua a leggere sotto
About the author

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
About the reviewerView full bio

Dr Colin Tidy, MRCGP
Medico di base, Autore medico
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy is an NHS Doctor, based in Oxfordshire.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Prossima revisione prevista: 13 Set 2028
15 Set 2023 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Iscriviti alla newsletter di Patient
La tua dose settimanale di consigli sulla salute chiari e affidabili - scritti per aiutarti a sentirti informato, sicuro e in controllo.
By subscribing you accept our Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.