Lesioni pigmentate della pelle
Revisione paritaria di Dr Toni Hazell, MRCGPUltimo aggiornamento di Dr Hayley Willacy, FRCGP Ultimo aggiornamento 10 Feb 2026
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Aggiungi alle fonti preferite su Google
Professionisti Medici
Gli articoli di riferimento professionale sono progettati per essere utilizzati dai professionisti della salute. Sono scritti da medici del Regno Unito e basati su prove di ricerca, linee guida del Regno Unito ed europee. Potresti trovare il Cancro della pelle melanoma articolo più utile, o uno dei nostri altri articoli sulla salute.
What are pigmented skin lesions?
Pigmented skin lesions can be considered as melanocytic neoplasms. The essential task is to exclude malignant melanoma. See also the separate Melanoma maligno della pelle e Tecniche di biopsia cutanea nella pratica generale articoli.
It is important to bear in mind that younger people in the UK are increasingly being affected by malignant melanoma, with over 900 diagnoses a year. This makes it the second most common cancer in those who are 25-49 years of age in the UK.1
Melanoma maligno
Image: a suspicious flat lesion, irregular in shape and pigmentation
Superficial spreading melanoma
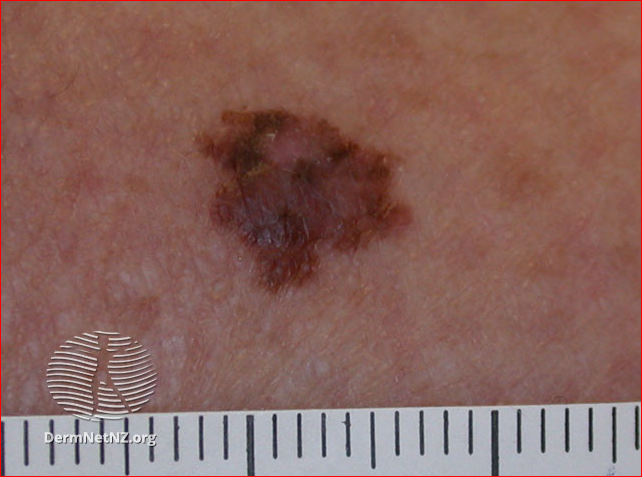
Superficial spreading melanoma image above:DermNet New Zealand. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 New Zealand License.
Melanomas may have a variety of colours, including tan, dark brown, black, blue, red and, occasionally, light grey.
When assessing melanomas, factor in risk factors2 including:
Family history of melanoma.
Personal history of melanoma.
Immunosoppressione.
Excessive UV exposure, including tanning beds.
7-point checklist
Use the 7-point weighted checklist for assessment of pigmented skin lesions:3
Major features of lesions (two points each):
Cambiamento di dimensione.
Forma irregolare.
Colore irregolare.
Minor features of lesions (one point each):
Diametro massimo 7 mm o più.
Infiammazione.
Essudazione.
Cambiamento di sensazione.
Lesions scoring three points or more in the 7-point checklist above are suspicious (if you strongly suspect cancer, any one feature is adequate to prompt urgent referral).
For low-suspicion lesions, undertake careful monitoring for change, using the 7-point checklist.
The National Institute for Health and Care Excellence (NICE) recommends ideally making measurements with photographs and a marker scale and/or ruler.
This guidance comes from the 2015 NICE guideline on detection of cancer. The guidance was updated in 2020, but there were no changes relevant to assessment and diagnosis of skin cancer.3
ABCDE
An alternative aide-mémoire to the 7-point checklist described below is the 'ABCDE' list:
Asimmetria.
Vorder irregular.
Colour irregular.
Diameter greater than 7 mm.
Evolving.
Melanoma vs normal mole
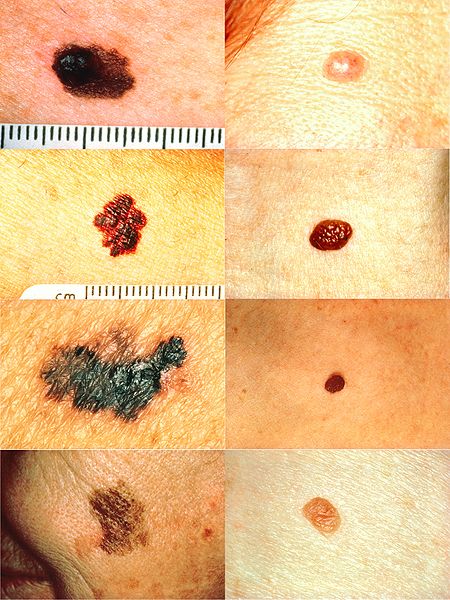
However, not all these features may be present and, if malignant melanoma cannot be excluded then excision biopsy is required.4
Change in size: naevi may change in size over years but any change over weeks or months is suspicious.
Change in colour:
Melanomas often show irregular pigment in a lesion, with shades of black, brown, grey and pink. In nodular melanoma (see below) the lesion is often black throughout.
Rarely, a melanoma can present as a non-pigmented red nodule (amelanotic melanoma), which is more likely on the hands and feet.
Change in outline: melanomas often show a geographical outline with a sharp cut-off from normal skin.
Itching may be a late sign and is often unreliable, as many benign naevi intermittently itch.
Bleeding is also a late sign and is often present in advanced melanoma.
Melanoma in women occurs more commonly on the extremities and in men on the trunk or head and neck but it can arise from any site on the skin surface.
Examination of suspicious lesions should include a thorough assessment for other suspicious skin lesions, palpation for regional lymph nodes and examination of the abdomen for enlarged liver and/or spleen.
Nodular melanoma
Informazioni importanti |
|---|
Nodular melanoma tends to lack the typical ABCDE melanoma warning signs and therefore may be diagnosed late with a much worse prognosis. Nodular melanomas tend to occur on the heads and necks of elderly sun-damaged men.5 A nodular melanoma is usually uniform in colour with early ulceration and bleeding. |
Image: pigmented lesion on an exposed area. It looks highly suspicious - the patient should be referred urgently
Nodular melanoma on an ear
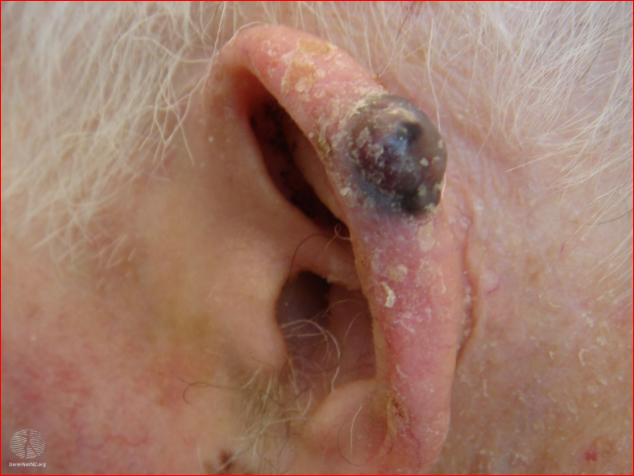
Nodular melanoma image above:
DermNet New Zealand. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 New Zealand License.
Multiple cutaneous melanomas
The incidence of multiple primary melanomas has been reported (depending on the study) from 1.1% to 20.4%.6The highest incidence of 20.4% was reported in Australia, while the highest incidence in Europe and North America was 18.1% in Austria and 8.6% in the US respectively.
The highest number of primary tumours in one individual was 13, and the mean number of primary tumours per individual ranged from 2.1 to 2.8.6
Lesions may be classified as synchronous if they present at the same time or within two months, or metachronous if the second melanoma presents later.
Other types of pigmented skin lesions
Intradermal naevi (common moles)
Also called common naevi. See also the separate Nevi intradermici e composti articolo.
Most adults will have approximately 30 moles which they have been acquiring from infancy. Naevi remain static whereas melanoma change in size, shape or colour over weeks or months. New common moles rarely develop after the age of 40 years and any that do are suspicious.
Typical features of common naevi are:
Symmetrical in area.
Even, brown colouring (light or dark).
Sharp margin.
<5 mm in diameter.
Profile varying from flat to pedunculated.
While an increased number of naevi is a strong melanoma risk factor, each individual naevus has a low risk of melanoma transformation, and most melanomas are non-naevus associated.7 Patients need careful skin monitoring, including baseline skin photography. Any lesion that starts to change colour, bleed, itch, be painful or increase in size needs excisional biopsy.
Dysplastic naevi (atypical moles)
Also known as dysplastic naevi. They are found in approximately 1 in 12 white people and do not usually become evident until puberty. Unlike melanoma, atypical naevi are usually symmetrical and do not have a sharp edge with geographical border; asymmetry and sharp-edged borders are clear signs of malignant transformation.8
Atypical moles are easily mistaken for malignant melanoma because of their:
Lack of symmetry.
Lack of sharp margin.
Size >6 mm.
Variation in colour within the lesion.
Image: atypical naevus
Atypical naevus

Atypical naevus image above:
DermNet New Zealand. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 New Zealand License.
Unlike common moles they continue to appear throughout life and occur in areas not often exposed to the sun - eg, buttocks. They are a strong, independent risk factor for malignant melanoma, conferring a 10-fold increased risk of malignant melanoma.8 This is especially the case when they are present in numbers (12% risk over ten years). Patients should be very careful with sunlight and undergo regular skin surveillance. Excision of dysplastic naevi is not performed routinely.
Congenital naevi (birth moles)9
Vedi il separato Nevo pigmentato congenito articolo.
Very large congenital naevi are known as giant naevi. Patients with large congenital naevi have an increased risk of developing malignant melanoma, often by the age of 10 years. These appear either within the lesion or as CNS melanoma. Treatment is either excision or close monitoring. Laser treatment is also available.
Blue naevus (blue moles)10
Vedi il separato Naevus blu articolo.
A blue naevus is a small blue or grey lesion, with an appearance similar to a mole. The diagnosis of blue naevus is generally clinical, made grossly, or with a dermatoscope, though biopsy and pathological evaluation are the gold standard for definitive diagnosis.
Image: blue naevus
Naevus blu
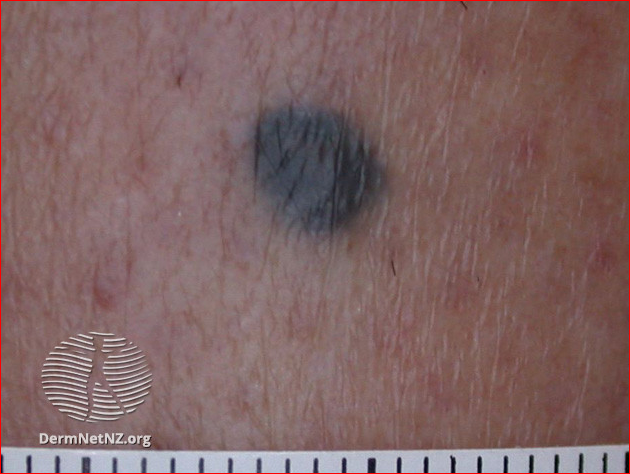
Blue naevus image above:
DermNet New Zealand. This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 New Zealand License.
Spitz naevus (pink or red moles)
Spitz naevi usually affect the face or limbs of young children. They initially grow rapidly but may then remain static for years. They often disappear spontaneously after a period of time.11
Epidermal naevus (birthmark)
Vedi il separato Nevo epidermico e le sue sindromi articolo.
Epidermal naevi may be congenital lesions or develop during the early years of life. They tend to grow during childhood and then stabilise during the teenage years. They may be localised to a small area or occur in more diffuse forms.
Epidermal naevus syndromes are a heterogeneous group of disorders characterised by the presence of one or more congenital hamartomatous ectodermal naevi of the skin with other organ involvement, including brain, eye and the skeleton.
Nevo di Becker: this is a form of epidermal naevus (birthmark). It usually appears around puberty as a hyperpigmented patch, most often found on the upper trunk or shoulders.
Halo naevus (halo moles)
Vedi il separato Nevo di Halo articolo.
Usually, these consist of a central uniformly pigmented naevus, usually round or oval in shape, with a surrounding area of depigmentation of uniform width from the naevus's edge.
Junctional naevus (flat moles)
Vedi il separato Nevo giunzionale articolo.
Junctional naevi are often quite darkly pigmented and are macular or very thinly papular with only minimal elevation above the level of the skin.
They are an acquired lesion and as they age they can change their characteristics to that of compound naevi.
Compound naevus (flat and raised moles)
Vedi il separato Nevi intradermici e composti articolo.
Compound naevi arise from a flat (junctional) naevus that exists earlier in life. Pigmentation may be uneven within the naevus but is usually symmetrically distributed.
They are usually of a round/oval shape and roughly 2-7 mm in diameter. They may exist with a variable degree of pigmentation and even be the same colour as the surrounding skin.
Sebaceous naevus (birthmark)
Vedi il separato Nevo sebaceo articolo.
Usually a single hairless patch (round or linear) is noted on the scalp at birth or shortly afterwards. The classic appearance is velvety tan or yellow-orange.
Verruca seborroica
Vedi il separato Verruca seborroica articolo.
A flat-topped or warty-looking lesion that appears to be stuck on to the skin. They are usually pigmented, sometimes deeply. They may even be black.
Aggiornamenti esclusivi per i professionisti sanitari
Rimani informato con gli ultimi aggiornamenti clinici, approfondimenti professionali e linee guida basate su evidenze. La newsletter Patient Pro seleziona contenuti essenziali per i professionisti sanitari—consegnati direttamente nella tua casella di posta.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.
Ulteriori letture e riferimenti
- Melanoma: valutazione e gestione; Linee guida NICE (luglio 2015 - ultimo aggiornamento luglio 2022)
- Melanoma and pigmented lesions; NICE CKS, luglio 2022 (accesso solo Regno Unito)
- Cancro sospetto: riconoscimento e invio; Linee guida NICE (2015 - ultimo aggiornamento aprile 2026)
- Melanoma tests; Ricerca sul Cancro UK
- Lu CT, Lin TL, Mukundan A, et al; Skin Cancer: Epidemiology, Screening and Clinical Features of Acral Lentiginous Melanoma (ALM), Melanoma In Situ (MIS), Nodular Melanoma (NM) and Superficial Spreading Melanoma (SSM). J Cancer. 2025 Sep 21;16(13):3972-3990. doi: 10.7150/jca.116362. eCollection 2025.
- Apostu AP, Ungureanu L, Halmagyi SR, et al; Multiple primary melanomas: A literature review. Medicine (Baltimore). 2023 Jul 28;102(30):e34378. doi: 10.1097/MD.0000000000034378.
- Zhang Y, Ostrowski SM, Fisher DE; Nevi and Melanoma. Hematol Oncol Clin North Am. 2024 Oct;38(5):939-952. doi: 10.1016/j.hoc.2024.05.005. Epub 2024 Jun 15.
- Baigrie D, Tanner LS; Dysplastic Nevi.
- Navarro-Fernandez IN, Mahabal GD; Congenital Nevus.
- Austad SS, Athalye L; Blue Nevus.
- Skin lesions, tumours and cancers; DermNet NZ
Informazioni sull'autoreVisualizza il profilo completo

Dr Hayley Willacy, FRCGP
Medico di base, Autore medico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dott.ssa Hayley Willacy era un medico di base del NHS che lavorava nel nord-ovest dell'Inghilterra, e si è ritirata dalla pratica clinica nel 2022 dopo 30 anni.
Informazioni sul recensoreVisualizza il profilo completo

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
La Dott.ssa Toni Hazell si è laureata presso la St. Mary’s Hospital Medical School e ha completato il suo VTS al Northwick Park Hospital.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Articolo disponibile anche in Inglese, Tedesco, Spagnolo, Francese, Italiano, Portoghese, Hindi, Ebraico, Arabo, and Svedese.
Next review due: 9 Aug 2030
10 Feb 2026 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Altro in dermatologia
- Eczema asteatosico
- Lesione da freddo
- Infezioni fungine delle unghie
- Nevo di Halo
- Porpora di Henoch-Schönlein
- Impetigine
- Nevi intradermici e composti
- Nevo giunzionale
- Melanoma maligno della pelle
- Infezioni cutanee micobatteriche
- Nocardia
- Eruzione polimorfa da luce
- Porfirie
- Iperpigmentazione post-infiammatoria della pelle
- Scottatura solare
- Sclerosi sistemica
- Tinea capitis
- Toxocariasi
- Eczema varicoso
- Vasculite