Fibrillazione ventricolare
Revisione paritaria di Dr Toni Hazell, MRCGPUltimo aggiornamento di Dr Hayley Willacy, FRCGP Ultimo aggiornamento 23 maggio 2023
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Aggiungi alle fonti preferite su Google
Professionisti Medici
Gli articoli di riferimento professionale sono progettati per essere utilizzati dai professionisti della salute. Sono scritti da medici del Regno Unito e basati su prove di ricerca, linee guida del Regno Unito ed europee. Potresti trovare il Ritmi cardiaci anomali articolo più utile, o uno dei nostri altri articoli sulla salute.
What is ventricular fibrillation?
Ventricular fibrillation (VF) is a cause of cardiac arrest and sudden cardiac death. The ventricular muscle fibres contract randomly causing a complete failure of ventricular function. Most cases of ventricular fibrillation occur in patients with pre-existing known heart disease (with myocardial fibrosis - scarring - having a role1 ) but the precise nature of the underlying cause of VF is not currently known.
How common is ventricular fibrillation? (Epidemiology)
VF is the most commonly identified arrhythmia in cardiac arrest patients and has been reported as present in 70% of cardiac arrests.2
The incidence of VF parallels the incidence of ischaemic heart disease, with a peak incidence of VF occurring in people aged 45-75 years.
Fattori di rischio
VF is most often associated with coronary artery disease and as a terminal event. VF may be due to acute myocardial infarction (MI) or ischaemia, or occur because of a chronic infarction scar.
When electrocardiogram documentation is available, it often shows that rapid VT precedes VF.
VF can occur during any of the following conditions or situations:
Antiarrhythmic drug administration.
Ipossia.
Ischemia.
Very rapid ventricular rates in the pre-excitation syndrome.
Electrical shock administered during cardioversion.
Electrical shock caused by accidental contact with improperly grounded equipment.
Competitive ventricular pacing to terminate ventricular tachycardia (VT).
VF can occur in healthy, young athletes after a blunt (non-penetrating) blow to the chest.3 This known as commotio cordis.
Presentation of ventricular fibrillation
Patients may have a history of chest pain, fatigue, palpitations and other nonspecific complaints.
There may be known diagnosis or suggestion of pre-existing heart disease - eg, coronary artery disease, cardiomyopathy, valvular heart disease, miocardite, congenital heart disease, long QT syndrome, sindrome di Wolff-Parkinson-White (WPW) or Brugada's syndrome.
Diagnosi differenziale
Arrhythmias associated with cardiac arrest are divided into two groups:
Shockable rhythms: VF and VT.
Non-shockable rhythms: asystole and pulseless electrical activity (PEA): see the separate article on Adult Cardiopulmonary Arrest.
Other causes of sudden collapse such as dissezione aortica e embolia polmonare.
Indagini
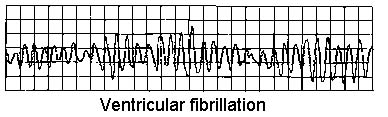
VENTRICULAR FIBRILLATION
Enzimi cardiaci (troponin).
Electrolytes, calcium and magnesium. Severe metabolic acidosis, hypokalaemia, hyperkalaemia, hypocalcaemia, and hypomagnesaemia are some of the conditions that can increase the risk for arrhythmia and sudden death.
Drug levels (eg, tricyclic antidepressants, digoxin). Most of the anti-arrhythmic medications also have a pro-arrhythmic effect.
Toxicology screen: drugs that can lead to vasospasm-induced ischaemia - eg, cocaine.
Ormone stimolante la tiroide (TSH): hyperthyroidism can lead to tachycardia and tachyarrhythmias.
ECG:4 evidence of MI, prolonged QT interval, short PR, WPW pattern or other conditions.
RX torace: signs of left heart failure, pulmonary hypertension.
Ecocardiografia: underlying structural abnormalities and cardiac dysfunction.
Nuclear imaging techniques:
Resting thallium (Tl) or technetium Tc 99m scintigraphy: assessing myocardial damage after MI.
Exercise nuclear scintigraphy: very sensitive in detecting the presence, extent and location of myocardial ischaemia.
Angiografia coronarica:
Cardiac catheterisation in patients who survive VF, to assess the state of ventricular function and severity and extent of coronary artery disease.
Coronary angiography identifies patients who may benefit from revascularisation by percutaneous coronary intervention (angioplasty) or coronary artery bypass grafting (CABG), and can also help identify coronary artery anomalies and other forms of congenital heart disease.
Management of ventricular fibrillation2
See the separate articles on Adult Cardiopulmonary Arrest e Defibrillazione e Cardioversione. Early defibrillation is essential to improve outcome.
Medical stabilisation
Patients who survive the initial episode of VF require a full evaluation of left ventricular function, myocardial perfusion and electrophysiological stability.
Careful post-resuscitation care is essential to survival because recurrence rates average at about 50%.
Treatment of myocardial ischaemia, heart failure and electrolyte disturbances.
Empirical beta-blockers are often given.
Most survivors of VF should be treated with implantable cardioverter defibrillators (ICDs).5 Transvenous ICDs can be placed with minimal morbidity and mortality.
Radiofrequency ablation: most cases of VF are not amenable to radiofrequency ablation and require ICD placement.
By itself, CABG only prevents recurrent VF if the ejection fraction is normal and ischaemia was the cause of the arrest. Even in these patients, ICDs are frequently placed after CABG.
Complications of ventricular fibrillation
Central nervous system ischaemic injury.
Myocardial injury.
Post-defibrillation arrhythmias.
Defibrillation injury to self or others.
Injuries from CPR and resuscitation.
Skin burns.
Morte.
Prognosi
Prognosis for survivors of VF strongly depends on the time elapsed between onset and medical intervention (prognosis is poor without intervention by 4-6 minutes after onset of VF) as well as on the particular aetiology for the VF.
Early defibrillation often makes the difference between long-term disability and functional recovery.6 If defibrillation is delivered promptly, survival rates as high as 75% have been reported.7
Death and disability after successful resuscitation correlate with the degree of central nervous system damage occurring during the event due to anoxia.
VF that occurs within the first 48 hours of the onset of acute MI has no bearing on prognosis, but VF that occurs more than 48 hours after acute MI is associated with a high rate of recurrence and a poorer prognosis.
After resuscitation, the prognosis is largely dependent on haemodynamic stability, early neurological recovery and duration of the resuscitation.
Education and training of non-healthcare professionals in basic life support and the use of automated external defibrillators in public places probably have the greatest impact on improving survival rates.
A major adverse outcome from a VF event is anoxic encephalopathy.
Aggiornamenti esclusivi per i professionisti sanitari
Rimani informato con gli ultimi aggiornamenti clinici, approfondimenti professionali e linee guida basate su evidenze. La newsletter Patient Pro seleziona contenuti essenziali per i professionisti sanitari—consegnati direttamente nella tua casella di posta.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.
Ulteriori letture e riferimenti
- Adult Tachycardia Algorithm; Resuscitation Council (UK), 2015 (updated 2021).
- Bezzerides VJ, Pu WT; Two sides of the same coin: new insights into mechanisms of ventricular fibrillation. Cardiovasc Res. 2021 Mar 21;117(4):983-984. doi: 10.1093/cvr/cvaa246.
- Ludhwani D, Goyal A, Jagtap M; Ventricular Fibrillation.
- Patel N, Pena C, Nesheiwat Z, et al; Ventricular fibrillation arrest after blunt chest trauma in a 33-year-old man, commotio cordis? BMC Cardiovasc Disord. 2022 Jun 3;22(1):252. doi: 10.1186/s12872-022-02689-4.
- Biblioteca ECG
- Defibrillatori cardioverter impiantabili e terapia di risincronizzazione cardiaca per aritmie e insufficienza cardiaca; Linee guida per la valutazione tecnologica NICE, giugno 2014
- Adgey AA, Spence MS, Walsh SJ; Theory and practice of defibrillation: (2) defibrillation for ventricular fibrillation. Heart. 2005 Jan;91(1):118
- Linee guida 2021 per il supporto vitale avanzato per adulti; Consiglio di Rianimazione UK
Informazioni sull'autoreVisualizza il profilo completo

Dr Hayley Willacy, FRCGP
Medico di base, Autore medico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dott.ssa Hayley Willacy era un medico di base del NHS che lavorava nel nord-ovest dell'Inghilterra, e si è ritirata dalla pratica clinica nel 2022 dopo 30 anni.
Informazioni sul recensoreVisualizza il profilo completo

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
La Dott.ssa Toni Hazell si è laureata presso la St. Mary’s Hospital Medical School e ha completato il suo VTS al Northwick Park Hospital.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Articolo disponibile anche in Inglese, Tedesco, Spagnolo, Francese, Italiano, Portoghese, Hindi, Ebraico, Arabo, and Svedese.
Prossima revisione prevista: 21 maggio 2028
23 maggio 2023 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Di più sulle malattie cardiovascolari
- Aneurismi dell'aorta addominale
- Rigurgito aortico
- Tumori cardiaci
- Riabilitazione dopo evento cerebrovascolare
- Cianosi
- Digossina e i glicosidi cardiaci
- Vertigini, capogiri e sensazione di svenimento
- Ecocardiografia
- Tetralogia di Fallot
- Soffi cardiaci nei bambini
- Palpitazioni cardiache
- Emergenze ipertensive
- Defibrillatori cardioverter impiantabili
- Stenosi mitralica
- Prolasso della valvola mitrale
- Cefalea primaria associata all'attività sessuale
- Prevenzione dell'ictus
- Tromboflebite superficiale
- Svenimento
- Criteri di Wells per l'embolia polmonare (EP)