Ginocchia valghe
Revisione paritaria di Dr Doug McKechnie, MRCGPUltimo aggiornamento di Dr Hayley Willacy, FRCGP Ultimo aggiornamento 15 giu 2023
Rispetta le linee guida editoriali
- ScaricaScarica
- Condividi
- Language
- Discussione
- Versione audio
- Aggiungi alle fonti preferite su Google
Le ginocchia valghe descrivono un angolo insolito delle gambe inferiori. Più comunemente è una forma normale durante lo sviluppo delle gambe dei bambini, ma occasionalmente nei bambini o negli adulti può causare problemi o avere una causa sottostante. La maggior parte dei bambini con ginocchia valghe supera questa condizione.
A colpo d'occhio
Knock knees is when your knees touch but your ankles are apart when standing.
It is a normal part of growth in children, usually from ages 2 to 8.
Most cases of knock knees correct themselves without treatment.
See a doctor if only one leg is affected, or if there is pain or difficulty walking.
You should also see a doctor if knock knees appear before age 2 or after age 8.
In questo articolo:
Scelte video per Sviluppo
Continua a leggere sotto
What are knock knees?
The medical term for knock knees is 'genu valgum' - genu meaning 'knee' in Latin, and valgum meaning 'bending outwards'. In knock knees, if the knees touch it is the lower leg which seems bent outwards. So if you have knock knees you are unable to stand with your knees AND your ankles together.
As children grow up, they tend to start off 'bow-legged'. This means if their feet are together, their knees are apart, leaving a diamond shape between the legs. This is normal in babies and toddlers until the age of about 2 years.
As the child's leg bones grow and develop, they then tend to take on a 'knock-kneed' shape. Now if their knees are together, their feet and ankles are apart. It tends to be most obvious around the age of 3 or 4 years, usually gradually improving to the correct position after that, as the child stands for longer periods of time. Knock knees are normal up to the age of 7 or 8 years, although the condition may last longer.
Valgus
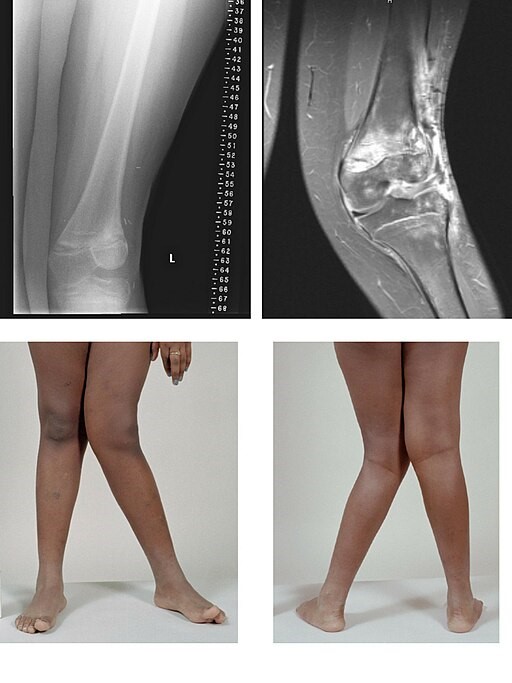
© BioMed Central, CC BY 2.0, via Wikimedia Commons
Do knock knees cause any problems?
Torna ai contenutiKnock knees in children do not cause problems. If the condition is severe, or caused by an underlying problem, it may cause pain or difficulty walking.
Continua a leggere sotto
Causes of knock knees
Torna ai contenutiIn most cases, knock knees are purely caused by the normal phase of growth and development. Occasionally - in either older children or adults - there can be an underlying problem causing the condition. For example:
Vitamin deficiency (particularly vitamin D deficiency causing rickets). Vitamina C and calcium deficiency can also affect the way bones grow.
Operations or injuries to the knee or legs.
Inherited (genetic) conditions which affect the way that the knees develop.
Do I need to see a doctor about knock knees?
Torna ai contenutiYou do not need to see a doctor if your child is at an age where having knock knees is normal (aged more than 2 years and less than 8 years) and if the deformity is not very severe. If your child lies on their back with their knees together, you can measure the distance between their ankles.
If it is less than 10 cm around age 4 years, this is likely to correct itself as they grow. If you take photos of your child every 3-6 months, standing with their knees together, you should see that the legs gradually become straighter from the age of 4 years or so.
See a doctor if:
Only one leg is affected.
Your child has knock knees before the age of 2 years or after the age of 8 years.
There is a larger gap between the ankles than that described above.
Your child has pain in the lower legs or knees.
Your child has problems walking or walks with a limp.
You develop knock knees as an adult.
Continua a leggere sotto
How are knock knees diagnosed?
Torna ai contenutiThe diagnosis of knock knees can be made by just looking at a child. If it is particularly severe, or if it occurs outside the normal age range, then further tests may be needed. This might include radiografie oppure esami del sangue.
The severity of the knock knees can be assessed by measuring the distance between the ankles when the child is standing with knees together. or by measuring other angles of the legs.
Treatment for knock knees
Torna ai contenutiIn most cases no treatment is needed. For children who develop knock knees as a normal part of their childhood growth, the condition corrects itself as they continue to grow. They do not need any special shoes or braces, and do not need to avoid any sporting activities. They do not need any physiotherapy or other special treatment.
If the condition is severe, or caused by an underlying problem, then treatment may be needed. This will then depend on the underlying condition, the severity of the deformity and the stage of growth that the child is in.
If the knock knees are caused by a metabolic problem, such as Vitamin D deficiency, the deformity may correct with vitamin replacement.
If the angle of bone growth is around 15-20 degrees in a child who is less than 10 years old, guided growth may be suitable to treat knock knees. Plates, or screws or staples may be implanted into the bone to aid correct growth.
Occasionally an operation to correct the deformity is needed. This is called an osteotomy and is usually followed by physiotherapy.
What is the outlook for children with knock knees?
Torna ai contenutiChildren who have knock knees as part of their normal growth pattern do very well without any medical assistance. Children who have an underlying condition can also do very well as long as their condition is recognised and treated. Complications only usually occur when an underlying condition is missed.
Scelte del paziente per Sviluppo

Salute dei bambini
Piede torto
Piede torto (anche chiamato talipes equinovarus) è una deformità del piede e della caviglia con cui un bambino può nascere. Non è chiaro esattamente cosa causi il piede torto. Nella maggior parte dei casi, viene diagnosticato dall'aspetto tipico del piede di un neonato dopo la nascita. Il metodo Ponseti è un trattamento ampiamente utilizzato per il piede torto. Questo trattamento dà buoni risultati per la maggior parte dei bambini. Se non funziona, la chirurgia può aiutare.
di Dr Doug McKechnie, MRCGP

Salute dei bambini
Disprassia
Il disturbo della coordinazione dello sviluppo (DCD), noto anche come disprassia, è una condizione comune che colpisce principalmente la coordinazione motoria - il modo in cui il corpo organizza ed esegue compiti legati al movimento. Può influenzare anche altre attività, inclusa la parola. La disprassia si manifesta in bambini e adulti. Disprassia significa scarsa coordinazione, ma il termine 'disprassia' è ampiamente usato per descrivere la disprassia dello sviluppo nei bambini. Gli operatori sanitari ora chiamano questa condizione disturbo della coordinazione dello sviluppo, per distinguerla da problemi simili (anch'essi chiamati disprassia) causati da altre condizioni mediche - ad esempio, problemi di movimento dopo un trauma cranico o un ictus. Tuttavia, in questa brochure useremo il termine comunemente usato 'disprassia' per riferirci al DCD infantile. Inoltre, la disprassia nei bambini viene talvolta chiamata dagli operatori sanitari 'disturbo specifico dello sviluppo della funzione motoria' (SDDMF).
di Dr Toni Hazell, MRCGP
Domande frequenti
At what age do knock knees typically develop in children?
Knock knees tend to become most noticeable around the age of 3 or 4 years. Before this, babies and toddlers up to about 2 years old are usually bow-legged.
Can adults develop knock knees?
While knock knees are commonly a normal part of childhood growth, adults can develop them due to underlying issues such as rheumatoid arthritis, osteoarthritis, obesity, or previous injuries or operations to the knee or legs. If an adult develops knock knees, it's recommended to see a doctor.
What is the typical progression of knock knees in children?
Children usually start bow-legged, then transition to knock-kneed, most visibly around ages 3-4. This typically improves naturally to a corrected position as they continue to grow and stand more, usually normalizing by age 7 or 8, though it can last longer.
Do knock knees always correct themselves without intervention?
In most cases, knock knees in children that are part of normal growth will correct themselves without any treatment. However, if they are severe, caused by an underlying problem, or occur outside the typical age range, treatment or medical assessment may be necessary.
Are specific exercises or physiotherapy needed for knock knees in children?
No, for children whose knock knees are part of their normal growth and development, special shoes, braces, physiotherapy, or other special treatments are generally not needed. They can also continue to participate in sporting activities without restriction.
Ulteriori letture e riferimenti
- Rerucha CM, Dickison C, Baird DC; Anomalie degli arti inferiori nei bambini. Am Fam Physician. 15 agosto 2017;96(4):226-233.
- Patel M, Nelson R; Genu Valgum.
- Soheilipour F, Pazouki A, Mazaherinezhad A, et al; The Prevalence of Genu Varum and Genu Valgum in Overweight and Obese Patients: Assessing the Relationship between Body Mass Index and Knee Angular Deformities. Acta Biomed. 2020 Oct 5;91(4):ahead of print. doi: 10.23750/abm.v91i4.9077.
Continua a leggere sotto
Informazioni sull'autoreVisualizza il profilo completo

Dr Hayley Willacy, FRCGP
Medico di base, Autore medico
MBChB (1992), DRCOG, DFFP, MRCOG (Part 1) MRCGP (2007), DFSRH (2013), MSc - medical education (2020)
La Dott.ssa Hayley Willacy era un medico di base del NHS che lavorava nel nord-ovest dell'Inghilterra, e si è ritirata dalla pratica clinica nel 2022 dopo 30 anni.
Informazioni sul recensoreVisualizza il profilo completo

Dr Doug McKechnie, MRCGP
Scrittore Medico
MA, MBBS, MSc, DRCOG, MRCP(UK), MRCGP(2021), FHEA
Il dottor Doug McKechnie è un medico di base del NHS che lavora a Londra. Lavora a tempo pieno in ambito clinico ed è anche Vice Responsabile del modulo di Pratica Clinica e Professionale presso la Scuola di Medicina dell'University College London.
Storia dell'articolo
Le informazioni su questa pagina sono scritte e revisionate da clinici qualificati.
Prossima revisione prevista: 12 maggio 2028
15 giu 2023 | Ultima versione

Chiedi, condividi, connettiti.
Esplora le discussioni, fai domande e condividi esperienze su centinaia di argomenti di salute.

Non ti senti bene?
Valuta i tuoi sintomi online gratuitamente
Iscriviti alla newsletter di Patient
La tua dose settimanale di consigli sulla salute chiari e affidabili - scritti per aiutarti a sentirti informato, sicuro e in controllo.
Abbonandoti accetti i nostri Informativa sulla Privacy. Puoi annullare l'iscrizione in qualsiasi momento. Non vendiamo mai i tuoi dati.